Despite a better understanding of the impact of local and systematic factors on anastomotic healing post-surgery, anastomotic leaks remain a common concern.
The rate of anastomotic leaks per surgery varies but is reported to be between 2.7-8.7%¹.
A successful anastomosis is a surgical connection between two structures and is commonly used on tubular structures, such as blood vessels or loops of the intestine.
One of the most severe bowel complications is an anastomotic leak, which occurs when fluid leaks from the surgical joint. In this article, we will look at the common risk factors for an anastomotic leak and the best practices to try to avoid them.
COMMON COLORECTAL PROCEDURES USING ANASTOMOSIS
There are several procedures that use anastomoses in the bowel:
![]()
METHODS OF ANASTOMOSIS
There are three anastomosis techniques that can be performed in the bowel, which are:
![]()
ANASTOMOTIC LEAK
What is it?
![]()
A leak of luminal fluid. It is one of the most serious complications of colorectal surgery².
Anastomotic leaks lead to the contamination of the abdominal cavity which can cause infection and if left untreated, patient mortality.
When does it occur?
An early anastomotic leak is defined as leakage within 30 days post-operation; however, evidence suggests that the majority of leakage occurs within one week of surgery³.
Within the first few days post-operation, fibroblasts from the submucosa layer are active and begin to deposit collagen. By day 5, the new tissue has been able to gain strength. By 4 weeks post-op, the reorganisation of collagen is almost finished, and wound healing is at 90%². As a result, it is more common for anastomotic leaks to occur within the first week of surgery.
What are the risk factors?
Although the causes of an anastomotic leak are not completely understood, there are a number of risk factors that can increase the chances of anastomotic leaks occurring. We have listed the most common risk factors and divided these into patient factors and surgical factors
Patient risks²
Medication use such as corticosteroids and immunosuppressants
Smoking or alcohol excess
Diabetes Mellitus
Obesity or malnutrition
Surgical risks²
Emergency surgery
Longer intra-operative time
Peritoneal contamination e.g from pus, faeces or GI content
Oesophageal-gastric or rectal anastomosis
Poor surgical technique
Potential Preventions?
There are no proven methods to stop anastomotic leaks from occurring, however, a good anastomosis requires freedom from tension, adequate blood supply and good surgical technique. An adequate blood supply can be affected by the patient, and the risk factors mentioned above can be attributing factor to this. However, good surgical technique and removing tension is something within surgical control.
Stapling Vs. Hand Sewn
There is some controversy around whether stapling or hand sewing results in better surgical outcomes, but there is no evidence that produces a definitive conclusion.
The widespread availability and use of stapling devices has changed colorectal surgery. In 1980, Knight and Griffen developed the “double-staple” technique, which is now widely accepted for anastomoses. Both linear and circular staplers can be used to conduct the double-staple technique, eliminating the need for a hand-sewn, distal purse string, which is sometimes difficult or even impossible to accurately place low in the pelvis⁴.
Despite there being no clinically significant difference in patient outcomes for stapling vs sewn procedures, studies have shown that stapled anastomoses took on average 22 minutes less operation time compared to sutured anastomoses (p=0.0001). This had a knock-on effect to both operational and overall hospital costs, providing a saving of 183 euros in operation costs and 496 in overall hospital costs⁵.
Single Vs Double-stapling Technique
In a prospective randomised trial examining single vs. double-stapling techniques, there was a trend in favour of double-stapling with a 2.8% rate of occurrence for leaks versus an 8.6% rate for the single-stapling method⁶. However, there is further data to suggest that the overlapping staples may be the cause of the anastomotic leaks in these occurrences.

CIRCULAR STAPLERS
Removing ‘Dog Ears’
Lateral intersecting margins or ‘dog ears,’ may increase the risk of anastomotic leak. A study conducted in 2000 compared 2 groups of double-stapled side to end anastomoses, performed using pig intestines⁹.
Group A consisted of 35 intestines with circular anastomoses and found that the burst pressure was 90 mmHg. On the other hand, group B consisted of 32 intestines with bilateral dog ears. The bursting pressure for group B, the bilateral group, was much lower at 60 mmHg and in 42% of the cases the first disruption occurred at the corner of the dog ear⁹.
It can be concluded that the intersections of double-stapled anastomoses are a lateral weak point and that using a single-stapler is a less effective for securing an anastomosis when compared to a circular stapler⁹.
Circular Staplers for an Anastomosis
A 2020 study analysed 154 patients with stage 0 to III rectal cancer who underwent curative laparoscopic low anterior resection. Perioperative factors and complications were compared between the circular stapling technique and the usual double-stapling technique¹⁰.
The circular stapling technique was performed on 110 out of 154 of the patients studied, and no anastomotic leaks were discovered. There were 3 instances of anastomotic leaks in the group of patients where the double-stapling technique was performed (p=0.011). The study concluded that the circular stapling technique was responsible for preventing anastomotic leaks in all patients with upper rectal cancer¹⁰.
Challenges with Staplers
Circular staplers have significantly reduced the rate of anastomotic leaks, however, there are still challenges. From 2011- 2018 the FDA had 41,000 individual medical device reports on surgical staplers and staples, including 366 deaths, 9,000 serious injuries and over 32,000 malfunctions⁸. The main causes for these cases were:
- Opening of the staple line or malformation of staples
- Misfiring
- Difficulty in firing
- Failure of the stapler to fire the staple
- Misapplied staples (e.g a user applying staples to the wrong tissue or applying staples of the wrong size to the tissue)
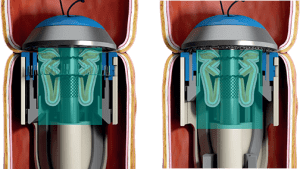
The Piston Effect

One challenge with circular staplers is the piston effect. The piston effect is an engineering challenge that is seen across industries with tubular structures, like train tunnels or the housing of a circular stapler.
Forced-air flow inside a tunnel or shaft caused by a moving object will lead to a build of pressure known as the piston effect. With staplers, this pressure build-up can cause the tissue to seep over the edge of the head of the stapler and cause the malformation of staples.
REVIEWING CIRCULAR STAPLERS
Touchstone saw the issues with circular staplers and decided to go back to basics, working with doctors to understand their biggest challenges during surgery.

Initially looked at the efficacy of the cutting blade which led them to design, a circular blade with a twisting action leading to a better across the stapler lines. This can be found in the CSC which has the rating blade feature.
Continuing from this they also looked to tackle the engineering concerns with circular stapler design and function. This combined approach led to the award-winning circular stapler design: the CST. The CST has taken circular stapling one step further, pushing innovation to ensure patient safety. Touchstone found that by significantly increasing the housing size by more than double, the CST eliminates the piston effect, creating clean and even doughnuts. Furthermore, an audible bell is rung when a staple is fired, to prevent from misfiring. The clear and concise steps required to fire these staplers, along with the clearly audible bell, signifying the firing and the automatic safety lock have contributed to patient safety and surgeon satisfaction.
We believe these changes can lead to a better anastomosis outcome and it warrants further investigation. Made with the aim to improve patient safety and help the surgeon make stronger and more secure anastomoses. However, as discussed, there are multiple causes for anastomotic leaks and while new innovations in circular stapling cannot completely remove these risks, they are a step in the right direction.
“Discover our surgical solutions designed to support anastomosis procedures and improve patient outcomes.”
References
1. Park, Jong Seob MD, Jung Wook MD Huh, Yoon Ah MD Park, Yong Beom MD Cho, Seong Hyeon MD Yun, Hee Cheol MD Kim, and Woo Yong MD Lee. “Risk Factors of Anastomotic Leakage and Long-Term Survival After Colorectal Surgery.” Medicine 95, no. 8 (February 2016).
2. Fang, Alex, Chao Wilson, and Melanie Ecker. “Review of Colonic Anastomotic Leakage and Prevention Methods.” Journal of Clinical Medicine 16, no. 9 (December 2020).
3. Li, Yi-Wei, Peng Lian, Ben Huang, Ming-He Wang, and Wei-Lie Gu. “Very Early Colorectal Anastomotic Leakage within 5 Post-Operative Days: A More Severe Subtype Needs Relaparatomy.” Sci Rep 13, no. 7 (January 2017).
4. Baran, J, SD Goldstein, and AM Resnik. “The Double-Staple Technique in Colorectal Anastomoses: A Critical Review.” Am Surg 58, no. 4 (April 1992).
5. Schineis, C, T Fenzl, L Aschenbrenner, L Lobbes, A Stroux, B Weixler, K Beyer, C Kamphues, M. E. Kreis, and J. C. Lauscher. “Stapled Intestinal Anastomoses Are More Cost Effective than Hand-Sewn Anastomoses in a Diagnosis Related Group System.” The Surgeon 19, no. 6 (May 2021).
6. Moritz E, Achleitner D, Hölbling N, Miller K, Speil T, Weber F. Single vs. double stapling technique in colorectal surgery. A prospective randomized trial. Dis Colon Rectum. 1991 Jun;34(6):495-7.
7. Lee, S, and B Ahn. “The Relationship Between the Number of Intersections of Staple Lines and Anastomotic Leakage After the Use of a Double Stapling Technique in Laparoscopic Colorectal Surgery.” Surg Laparosc Endosc Percutan Tech 27, no. 4 (August 2017).
8.https://www.fda.gov/medical-devices/letters-health-care-providers/safe-use-surgical-staplers-and-staples-letter-health-care-providers.
9. Roumen, Rudi M. H., PHD, Frank Rahusen, and Marc. M. D. Wijnen. ‘Dog Ear’ Formation after Double-Stapled Low Anterior Resection as a Risk Factor for Anastomotic Disruption.” Diseases of the Colon & Rectum 43, no. 4 (April 2000).
10. Villanueva-Sáenz E, Sierra-Montenegro E, Rojas-Illanes M, Peña-Ruiz Esparza JP, Martínez Hernández-Magro P, Bolaños-Badillo LE. Doble engrapado en cirugía colorrectal [Double stapler technique in colorectal surgery]. Cir Cir. 2008 Jan-Feb;76(1):49-53. Spanish.